Background and Aims
The Global Burden of Disease Study 2016 confirmed that the high prevalence of pain and pain-related diseases is the leading cause of disability and disease burden globally. Pain is the most common reason patients consult primary care providers in the United States. According to recent literature, over 40% of the adult Americans, an estimated 100 million people, live with chronic or recurrent pain. Ongoing research is needed to evaluate the impact of pain and identify alternative multimodal strategies to existing treatment approaches as a means to reduce pain severity, pain interference, and to improve a patient’s quality of life.
A proper treatment strategy should employ therapies providing optimal benefit and minimal harm. Chronic pain, which is categorized as either nociceptive (caused by damage to tissue or inflammatory stimuli) or neuropathic (damage to somatosensory nervous system), is commonly treated by oral opioids and other oral analgesics. Despite the extensive use of opioids and other oral medications, a large percentage of pain patients do not achieve adequate pain relief and traditional oral medications are often associated with prolonged healing and undesirable and negative side effects.
Alternative evidence-based multimodal approaches of pain management have become increasingly widespread. These therapies include use of combination pharmacotherapy, which target both central and peripheral nociceptive mechanisms, and non-pharmacological interventions. Incorporation of nanotechnology into the development of novel treatments has shown to have positive effects on patients. Topical analgesics, including pain relief patches, is a potentially valuable strategy in the management of a variety of conditions associated with mild, moderate, or chronic pain, including musculoskeletal pain and various neuropathic pain disorders.
The purpose of this minimal risk, observational study was to evaluate patients with mild, moderate, or chronic pain and evaluate perceptions of pain treatment and associated symptoms with the use of a novel, non-drug, and nanotechnology-based topical pain-relieving patch via validated scales (e.g., Brief Pain Inventory (BPI)), subject, and clinician reported surveys over the course of 30 days.
Methods
This analysis of the PREVENT IRB-approved study evaluated the efficacy of a topical pain-relieving patch (Kailo Pain Relieving Patch (Pain Relief Technologies, USA) in reducing Brief Pain Inventory (BPI) scores in patients experiencing mild, moderate, or chronic pain (Figure 1). The Treatment Group (TG) of 128 adult patients (89 females,39 males) with arthritic, neuropathic, or musculoskeletal pain received patches for 30 days. A Control Group (CG),of 20 adult patients (15 females, 5 males) did not initially receive the patch, and then crossed over to the Crossover Treatment Group (CROSSG), Surveys were administered to all patients at baseline, 14 days, and 30 days to assess changes in pain severity and interference by BPI Short Form. Changes in oral pain medication use, side effects and satisfaction with patch use were also assessed.
FIGURE 1:

Results
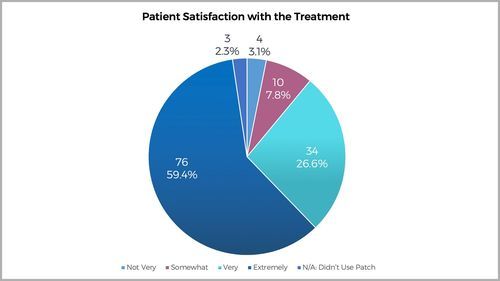
Treatment group paired data were collected. Over 30 days, treatment group mean BPI Severity score decreased 61% (4.9 to 1.9/10;P< .001) and mean BPI Interference score decreased 61% (3.8 to 1.5/10;P< .001) The control group showed an increase in both BPI Severity of 23% (3.0 to 3.7/10) and BPI Interference Score of 58% (1.2 to 1.9/10). After crossing over to treatment, patients in the crossover group reported a decrease in BPI Severity score of 76% (3.7 to .9/10) and a decrease in BPI Interference score of 79% (1.9 to .4/10) (Figure 2). No side effects of treatment were reported. After 30 days, 91% of patients reported “less” or “a lot less” usage of oral medications. 86% of patients were very/extremely satisfied with the patch and preferred the pain-relieving patch to oral medications (Figure 3). Results also showed Quality of Life (QoL) improvements in mood, relations with other people, sleep, walking ability, and enjoyment of life.
FIGURE 2:
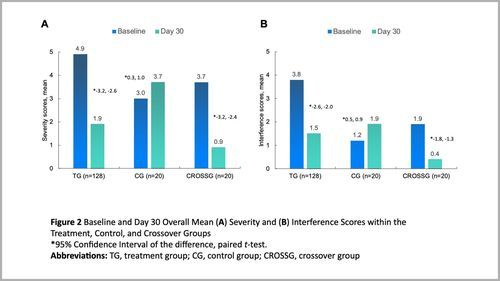
FIGURE 3: